Oral Tie Release, What Parents Should Know Before and After Treatment

Oral tie release is a procedure used to free a tight band of tissue in the mouth when that tissue is clearly limiting normal function. In babies, that usually means trouble with latch, milk transfer, or painful breastfeeding. In older children, the concern may involve tongue movement, oral hygiene, or day to day mouth function. The most important point for readers is this. A visible tie alone is not the reason for treatment. Current guidance from pediatric dental and breastfeeding groups says treatment decisions should be based on function, not appearance alone.
Table of Contents
What Oral Ties Actually Are
An oral tie involves a frenulum, which is a normal fold of tissue inside the mouth. The lingual frenulum sits under the tongue. The labial frenulum connects the upper lip to the gum. Buccal frenula connect the cheeks to the gums. These tissues are normal parts of oral anatomy, but in some children a restrictive frenulum can limit movement enough to cause real problems. Cleveland Clinic notes that tongue tie, or ankyloglossia, is diagnosed when a restrictive lingual frenulum limits tongue function. The Academy of Breastfeeding Medicine goes further and calls tongue tie a functional diagnosis, which means the anatomy must be linked to symptoms before surgery is considered.
Types of Oral Ties
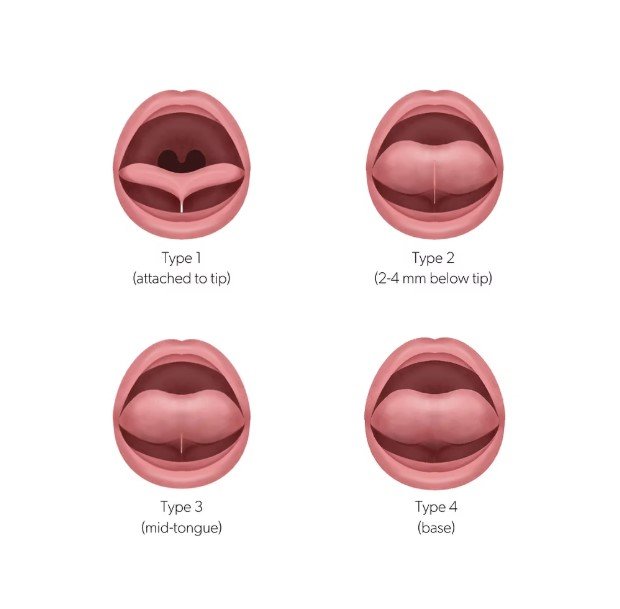
Tongue tie is the best known form of oral tie. It affects the underside of the tongue and may restrict tongue elevation, extension, and effective movement during feeding. Lip tie refers to the upper labial frenulum. Buccal tie refers to cheek attachments. These terms are common online, but the evidence behind them is not equal. The strongest support for oral tie release is for a restrictive sublingual frenulum in a breastfeeding infant when skilled feeding support has not solved painful latch or poor milk transfer. The evidence for upper lip tie release is weaker, and the Academy of Breastfeeding Medicine states that surgery on the upper labial frenulum cannot be recommended to improve breastfeeding. The same statement says buccal tie surgery should not be performed for breastfeeding concerns.
Signs of Oral Ties in Babies
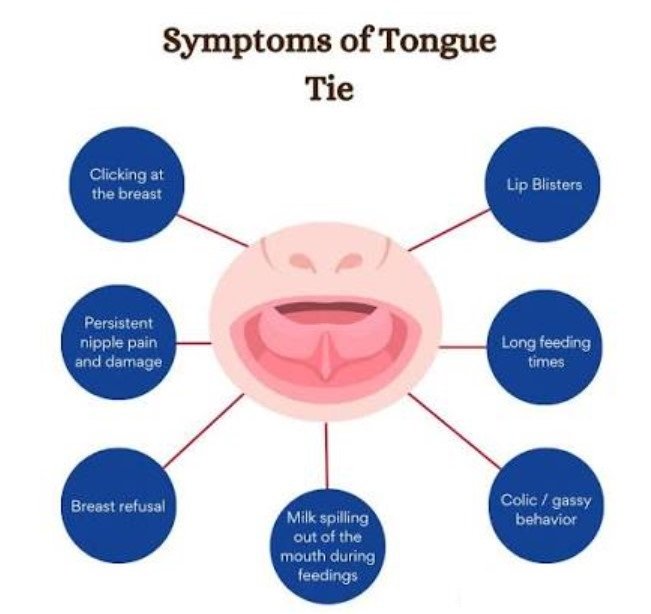
Parents usually start looking into oral tie release when feeding feels hard from the start. Common signs include poor latch, clicking at the breast, frequent unlatching, long feeds, weak milk transfer, poor weight gain, sore nipples, and pain during nursing. These signs matter, but they are not specific to tongue tie. Cleveland Clinic points out that these symptoms can happen for many reasons, which is why a full feeding assessment matters before anyone recommends a procedure. In plain terms, oral ties can be one cause of feeding trouble, but they are not the only cause.
Signs in Older Children
Older children may show different concerns. Families may notice limited tongue movement, trouble clearing food from the teeth, oral hygiene problems, or frustration with mouth movements. Some parents worry about speech. Current evidence does not support doing a frenotomy in infancy just to prevent later speech problems. Cleveland Clinic states that research does not show an association between tongue tie and speech disorders strong enough to justify preventive surgery in babies, and older children with speech concerns are more likely to benefit from speech therapy than from a frenotomy done for prevention alone.
When Oral Tie Release Helps
Oral tie release can help when there is a clear match between structure and function. The Academy of Breastfeeding Medicine says surgical release of a restrictive sublingual frenulum can be effective when maternal nipple pain or poor milk transfer cannot be corrected in a timely way through conservative measures. Cleveland Clinic says the procedure may help a baby latch better for breastfeeding. The American Academy of Pediatrics recommends reserving frenotomy for cases where significant functional impairment is present and nonsurgical measures have already failed. That is the right framework for families. Start with function. Use support first. Move to the procedure when symptoms remain significant.
Also Read: Oral Surgery Aftercare Instructions: A Comprehensive Guide
When Support Comes Before Surgery
Many babies improve without surgery. Cleveland Clinic notes that changes to breastfeeding position and latch often help, and lactation consultants can play a key role in solving feeding problems. The American Academy of Pediatrics recommends early identification of feeding problems and collaboration with lactation consultants and other specialists. That means a good provider should not rush straight to clipping. A careful plan often includes observing a full feed, checking latch, reviewing milk transfer, and ruling out other reasons for pain or poor weight gain.
How the Procedure Works
The procedure most parents hear about is a frenotomy. Cleveland Clinic describes it as a quick, in office procedure that usually uses scissors and does not require anesthesia in infants. The goal is simple. Release the restriction so the tongue can move more freely. In different clinics you may also hear the terms frenectomy or frenuloplasty. The name can vary by technique and how much tissue is addressed, but the purpose stays the same. The provider is trying to improve function, not just change how the tissue looks.
Laser or Scissors, What Parents Should Know
Parents often ask whether laser oral tie release is better than scissors. Current evidence does not clearly show that one tool is superior for all cases. The Academy of Breastfeeding Medicine says scissors remain the gold standard for treating a classic tongue tie in breastfeeding infants and notes that there are no published studies directly comparing the surgical instruments or methods used for frenotomy. That means families should focus less on the device and more on the provider’s assessment, experience, follow up care, and ability to support feeding after the release.
Benefits Parents Can Realistically Expect
The potential benefit is not perfection overnight. The main benefits are often better latch, less nipple pain, improved milk transfer, and better tongue movement. The Academy of Breastfeeding Medicine says frenotomy can increase maternal comfort and breast milk transfer in the right cases. Cleveland Clinic says the procedure may help babies latch better. But the benefit depends on the diagnosis being right in the first place. A baby with feeding difficulty from another cause will not improve just because a frenulum was clipped.
Risks, Side Effects, and Limits
Oral tie release is generally considered safe when done for the right reason, but it is still a procedure and it has limits. Cleveland Clinic lists rare complications such as bleeding, infection, scarring, feeding aversion, and injury to saliva ducts. The American Academy of Pediatrics says the procedure is safe and poor outcomes are rare, but it still recommends using it selectively. Families should know both parts. The procedure is usually low risk, but it is not something to do casually, and it is not a fix for every feeding problem.
Oral Tie Release Recovery, What to Expect
Recovery is usually short, but the first few days can feel stressful for parents. NHS aftercare guidance says some babies may be unsettled for a couple of days after frenulotomy. Frequent feeds help soothe the area and support healing. The same guidance notes that parents may see a pink diamond shaped wound under the tongue at first, followed later by a white or yellow blister like patch as healing continues. This appearance is often normal. A small amount of bleeding can happen, but any bleeding should usually stop after feeding.
Aftercare Tips That Actually Help
The most useful aftercare advice is simple. Feed often. Keep the baby comfortable. Watch healing. Get help early if something seems wrong. NHS guidance recommends frequent feeds after the procedure, and says cuddling, massage, and feeding can help settle an unsettled baby. If a baby is older than eight weeks, age appropriate paracetamol may be used based on medical advice. Parents should pay attention to feeding quality in the next two to three weeks, since scar tissue can occasionally reduce the benefit of the release.
Do Stretches Prevent Reattachment
This is one of the most confusing parts of oral tie release care. Many clinics still recommend stretches or wound opening exercises. But major medical groups now urge caution. The Academy of Breastfeeding Medicine says evidence is lacking to support post procedural stretching or manual manipulation near the incision. The American Academy of Pediatrics also advises avoiding post frenotomy stretching exercises where parents repeatedly open the wound to prevent reattachment. This does not mean every clinic follows the same plan. It means parents should ask for a clear, evidence based explanation before starting any painful home routine.
When to Call Your Provider

Parents should contact their provider if the wound becomes swollen, red, or inflamed, if the baby has a temperature of 38 degrees Celsius or higher, if feeding gets worse, or if the baby seems reluctant to feed, unusually sleepy, or persistently irritable. Those red flags are listed in NHS aftercare guidance and give families a practical safety check. The goal after oral tie release is better feeding and better function. If symptoms are moving in the opposite direction, the child needs reassessment.
Also Read: Order of Oral Care: Best Routine for a Healthier Smile
Why Choosing the Right Provider Matters
Families searching oral tie release near me often focus on the procedure itself. A better question is this. Who will assess feeding thoroughly, explain the evidence honestly, and support recovery after treatment. Good care usually involves more than one person. The American Academy of Pediatrics recommends collaboration with lactation consultants, speech language pathologists, and other specialists when needed. That kind of team approach is often what separates rushed treatment from thoughtful treatment.
The Bottom Line on Oral Tie Release
Oral tie release can be helpful, but only when it is used for the right problem. The current evidence supports frenotomy most clearly for a restrictive tongue tie that is causing significant breastfeeding problems and has not improved with conservative care. Not every visible tie needs treatment. Lip tie release has weak evidence for breastfeeding benefit, and buccal tie release is not recommended for breastfeeding concerns by the Academy of Breastfeeding Medicine. Parents get the best results when they choose a provider who looks at the whole feeding picture, explains benefits and limits clearly, and offers follow up after the procedure. If feeding is painful, milk transfer is poor, or your baby is not gaining well, the best next step is a skilled assessment, not guesswork.
Authority referral links used in this article
- American Academy of Pediatric Dentistry, Policy on Management of the Frenulum in Pediatric Patients.(AAPD)
- American Academy of Pediatrics guidance on tongue tie and breastfeeding concerns. (healthychilderen)
- Academy of Breastfeeding Medicine Position Statement on Ankyloglossia in Breastfeeding Dyads.
- Cleveland Clinic clinical overview of tongue tie and frenotomy.
- NHS frenulotomy aftercare guidance for parents.


